Ebola Outbreaks Research
Ebola: Infographic
Download and share our infographic summarizing outbreaks, occurrences and research on Ebola (Last updated November 11, 2015)
What is Ebola?
The Ebola virus causes the often fatal Ebola virus disease (EVD) previously known as Ebola hemorrhagic fever. It can be transmitted from wild animals, such as bats, to humans and then caught from close contact with body fluid from infected individuals. There are 5 identified strains of Ebola virus: Zaire, Bundibugyo, Sudan, Reston and Taï Forest.
The virus enters the body via cuts or through exposed mucus membranes such as the eyes, and symptoms usually occur 2-21 days later. The infectious period occurs with the symptoms, which are fever, muscle pain, headache, sore throat, nausea, diarrhea, rash, kidney and liver problems.
The final stages involve external bleeding such as from the gums and in the stools. The virus can also remain in semen for 7 weeks after recovery from infection. Moreover, it can spread via breast milk and through contact with an infected deceased individual (Source: World Health Organization (WHO)).
Ebola outbreaks
Ebola outbreaks have tended to occur in Africa, and spread between countries via travel. The outbreak in Nigeria in 2014 occurred from just one infected Liberian air traveller who introduced the virus on 20th July, causing 8 deaths. Subsequently, Nigeria was declared Ebola free on the 20th October 2014.
There is currently no definitive cure for an Ebola infection, although early intervention techniques such as rehydrating can improve survival rates. Infection control efforts are focused on limiting the spread of the virus after an outbreak occurs.
This is achieved through engaging with the communities about isolating infected individuals, tracing contact with others and using surveillance techniques such as screening for infections at airports. Laboratory tests on infected individuals find low platelet/white blood count and high liver enzymes. However, diagnosis is difficult, and often requires advanced medical laboratory detection techniques such as ELISA, antigen capture, serum neutralization, Real-Time PCR, EM and viral cell culture.
Ebola species, including the number of deaths and cases identified from previous outbreaks
The virus responsible for the 2014 outbreak was the Zaire species, which has been identified as the most commonly occurring species in previous outbreaks (Source:WHO)(Fig.1A). Zaire has also been the cause of the highest number of cases and deaths between 1979 and 2012. The fatality percentage represents the percentage of people who die after contracting the virus, and Zaire has the highest at 69%, followed by Sudan at 53% (Fig. 1B). These figures suggest that the Zaire species of Ebola is the most virulent, and therefore requires further research. The Ebola outbreak (Zaire species) of 2014 has become larger than all previous Ebola outbreaks combined since its discovery in 1976. Ebola cases have historically been identified from Sudan, Democratic Republic of Congo, Gabon, Uganda, and Congo. Currently the three most affected countries in 2014 are: Sierra Leone, Liberia and Guinea, which do not have any previous history of Ebola cases. The closest previous incidence was one case of Ebola in Cote d'Ivoire in 1994, where the individual recovered. This lack of experience and facilities for controlling the spread of the virus has been a major factor contributing to the size of this outbreak. Furthermore, the low survival rates for Zaire heavily contribute to the increasing number of deaths during the current epidemic.
A
|
B
|
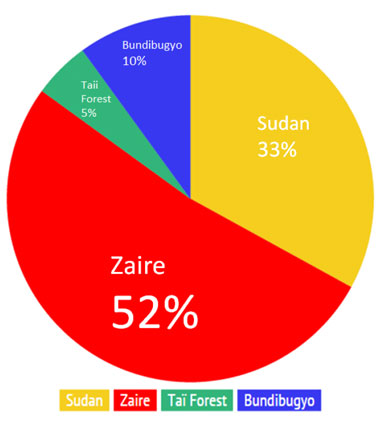
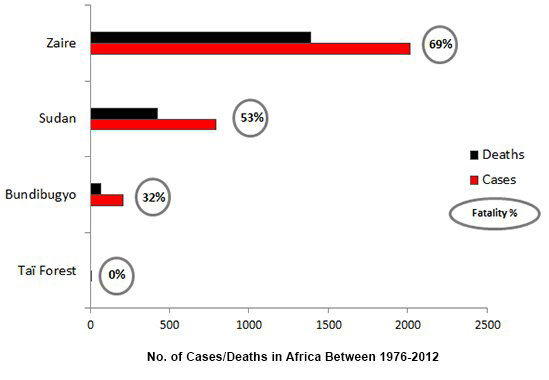
Figure 1. A. The total percentage occurrence of Ebola species, which have been implicated in an outbreak since 1979. This information has been adapted from WHO chronology outbreak data. B. The breakdown of total deaths, and cases, with the fatality percentages for Zaire, Sudan, Bundibugyo and Taï Forest species between 1976 and 2012.
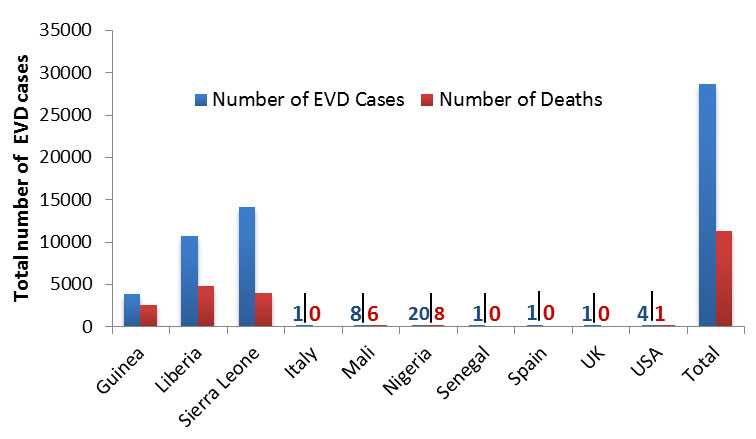
Due to the scale of deaths (over 11,000) the 2014 outbreak in Sierra Leone, Liberia and Guinea, was declared a “Public Health Emergency of International Concern" by the WHO Director on August 8, 2014. As of November 1, 2015, there have been over 28,000 confirmed, probable, and suspected Ebola cases spanning ten countries, including Spain, United Kingdom and the United States of America (Figure 2).
Total number of Ebola cases and deaths wordwide as of November 1, 2015
|
Figure 2. Total number of confirmed, suspected and probable Ebola cases and deaths as of November 1, 2015. This data was adapted from the WHO situation summary report on Ebola data and statistics published November 6, 2015.
Future prevention and research
Currently there are no licensed Ebola vaccines, although blood transfusion from an Ebola survivor can improve the survival rate of an infected individual. Two potential Ebola vaccines are currently being investigated, and are undergoing human safety testing. More research on other potential treatments are being considered, which include blood products, immune therapies, and drug therapies.
Research and development into easier diagnosis of Ebola using a rapid diagnostic kit is being conducted by Corgenix Medical Corporation (OTC BB: CONX.OB). In March 2015 the company announced a partnership with Fio Corporation to combine two existing technologies to support the current Ebola outbreak. One is a test that can detect the Ebola virus within minutes, and the other is a mobile device that can analyze and upload results to a central data system. Current Ebola tests are biological hazards, and often have to be sent away for laboratory tests. The availability of a field lab test for Ebola would enable much quicker responses to future epidemics, allowing for early intervention to limit the spread of the virus.
The NIH is an important source of funding for research and development into infectious diseases, and they are funding category 4 biohazards such as Ebola and Marbug with grants worth $101 million in 2011, which fell to $96 million in 2013. Notably, the NIH recently launched the largest controlled study of Ebola survivors to date, in partnership with researchers in Liberia. The goal of the study is to better understand the long-term health consequences of Ebola virus disease.
There is also funding being allocated to researching the outbreak response so that we can learn lessons and apply them to future Ebola epidemics. A proportion of funding will be allocated from a pot of $10.5 million which comes from Research for Health in Humanitarian Crises (R2HC), which aims to build evidence to support public health interventions in future humanitarian crises.
The Wellcome Trust offers support for research which could help contain the current Ebola epidemic and future outbreaks. Since the beginning of the outbreak, they have committed more than £10 million through their emergency Ebola research funding initiative. The initial emergency research involved how to improve preventing, containing and treating the disease. Investigation on the ethical challenges of testing experimental treatments on patients who are directly involved in an epidemic is also being conducted. The Wellcome Trust is calling for research proposals for testing experimental therapies and vaccines. They will also fund $64 million into the development of African health researchers.
It is likely that the scale of the current 2014 Ebola epidemic will initiate further research into preventing future outbreaks. The treatment of Ebola patients in Western countries is also likely to increase financial support for research into a vaccine to prevent the world wide spread, and to provide a treatment to cure Ebola virus disease.
Last updated: November 11, 2015.
Important Update
Read our Ebola Update - 'Does the ebola virus ever go away' Blog for more information.