The Cancer-Therapy Arms Race
- Feb 03, 2022
- 5 min read
- Grace Gregory, PhD
In this guest blog, Grace Gregory discusses Non-small Cell Lung Cancer (NSCLC), some of the different treatment approaches being used, and why finding the most appropriate treatment for NSCLC isn’t always straightforward.
We are under attack! Over 2.2 million cases of lung cancer were reported in 2020 with NSCLC accounting for 85% of diagnoses (Sung et al. 2021, Blandin Knight 2017). But how can we beat this enemy? The answer lies in the mechanisms underpinning NSCLC.
Cells communicate with each other through molecular signals which can be misinterpreted in cancers, so how can we prevent this? Shoot the messenger! The signals are received by proteins found on the cell surface called Epidermal Growth Factor Receptors (EGF Rs) and are commonly mutated in NSCLC patients (Cross et al. 2014). By shooting the EGF R messenger with specific EGF R-targeted therapies, we may be able to prevent this. However, creating effective drugs for NSCLC is not as simple as it seems, as the adversary has a trick up its sleeve…
The Enemy Emerges
In healthy tissues, EGF Rs are our allies. On a cell’s outer membrane, these proteins are activated after receiving a messenger ligand such as EGF. Below the cell’s surface, their internal domains awaken downstream proteins to elicit growth for healthy tissue repair. However, a traitor appears in cancerous tissues. Over 60% of NSCLC patients have pathogenic gain of function mutations that allow EGF Rs to become active even without stimulation. This overactivation signals the cells to grow out of control to form a tumor (Tamura et al. 2014). Are we becoming outnumbered?
The Ongoing Battle
To combat this, there are 36 FDA-approved drugs for NSCLC, with 47% of these being small molecule inhibitors. First-generation drugs such as gefitinib were used to quell the enemy by reversibly binding to EGF Rs (Yamaoka et al. 2018). However, cancer cells fought back by gaining resistance to reversible inhibitors, starting the first battle in the “Cancer-Therapy Arms Race”.
To get ahead, scientists developed second-generation drugs, such as afatinib, to bind irreversibly to EGF Rs preventing their traitorous overactivation. It was highly effective in preventing tumor growth, however NSCLC cells once again gained an advantage, with up to 60% of cases acquiring resistance in just 9–14 months and therefore limiting therapy effectiveness (Nan et al. 2017, Maemondo et al. 2010). The enemy’s secret was a threonine to methionine point mutation (T790M) that prevented afatinib binding through steric hindrance at the ATP binding site of the EGF Rs.
Our Newest Weapon
Heading into “No Man’s Land”, the race was on to create a new third-generation inhibitor for NSCLC treatment. The enemy had the new T790M mutation that it used like a forcefield to prevent our current drugs from working. For our next drug in the arsenal against these cancers, the action had to be specific and irreversible to EGF R proteins with the T790M mutation (Cross et al. 2014). The weapon came in the form of osimertinib, a third-generation inhibitor and the first of its kind (Figure 1).
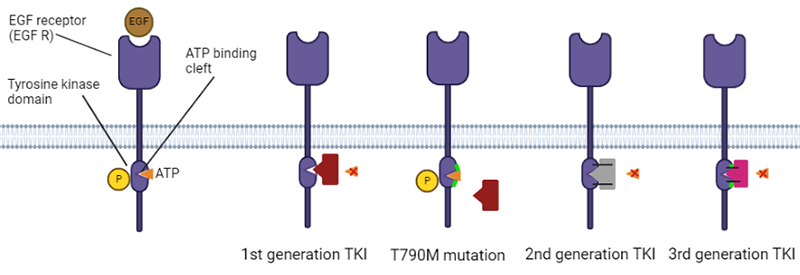
Fig. 1. Mechanism of tyrosine kinase inhibitors (TKIs) and overcoming the T790M mutation. 1st generation TKIs (red shape), like gefitinib, reversibly bind to EGF R to prevent ATP (orange triangle) binding. However, the T790 mutation (shown as a green line) is able to overcome this inhibition. 2nd generation TKIs (grey shape) have irreversible covalent binding to EGF R (shown by solid lines) but this can be again overcome by the T790M mutation, while 3rd generation TKIs (pink shape), like osimertinib, can irreversibly bind to EGF Rs with/without the T790M mutation.
Osimertinib has an astounding 200-times greater potency towards mutant EGF Rs compared with our healthy EGF R allies. This dramatically reduces the side effects seen in previous NSCLC treatments. To add to this arsenal, osimertinib showed it had the power to defeat EGF Rs, both with and without the T790M mutation, indicating it could replace first and second-generation therapies altogether (Takeda and Nakagawa 2019). Furthermore, treatment of NSCLC tissue with osimertinib as a first line defense showed that we could reduce the likelihood of the development of these T790M super soldiers. This was a great advantage over first and second-generation drugs such as gefitinib and afatinib. Could osimertinib be our secret weapon?
Surveying the Battlefield
Before running headfirst into battle, preliminary testing was done in mice. The first mouse model had NSCLC without the devious T790M mutation. Reduction in tumor volume confirmed that osimertinib was an effective replacement for first-generation drugs. The second model contained the T790M mutant EGF Rs. This determined that osimertinib was also very effective against the resistant NSCLC tumors (Cross et al. 2014), which was confirmed in a further study (Jiang et al. 2018). These results suggested osimertinib was ready to be used on the battlefield against a host of human NSCLCs.
Waging War
After promising results in mouse models, it was time for NSCLC in humans to feel the full force of osimertinib. Proof of concept was confirmed in two patients with NSCLC harboring the T790M mutation, one of which was acquired during prior treatment with gefitinib (Cross et al. 2014). Phase 1 trial patients were prescribed osimertinib once daily and tumor shrinkage was assessed. By the fifth scan, patients A and B had seen 52% and 59% tumor shrinkage respectively (Cross et al. 2014). Strikingly, these previously untreatable patients showed 9 months of positive drug-response and 11 months of progression-free survival. Were we winning this war?
Falling at the Front Line
Celebrations may have come too early for us as the enemy evolved its latest evasion tactic. After 11 months of successful osimertinib treatment, the two patients began to experience disease progression once more (Cross et al. 2014). Our secret weapon, osimertinib, binds EGF Rs just opposite the T790M mutation, but was it possible that these EGF Rs gained a secondary mutation to yet again put up a forcefield against our attacks? The scientists studying Patients A and B had never seen resistance to osimertinib due to novel mutations but could not investigate this further (Cross et al. 2014). The lack of biopsies and sequencing of the two patients’ resistant tumors limited this study, as this could have given us a peek behind enemy lines. Once again, NSCLC had gained an edge in battle, this time over third-generation EGF R inhibitors.
New Plan of Attack
Despite its success, osimertinib had an Achilles’ heel. Less than a year after its prediction, an acquired C797S mutation opposite T790M on EGF Rs was confirmed in six patients which provided osimertinib-resistance (Thress et al. 2015). If NSCLC cells can gain resistance through non-T790M mechanisms, then osimertinib becomes ineffective. Regardless of this setback, osimertinib became FDA-approved as it vastly improved progression-free survival of NSCLC patients and clinical trials showed its efficacy over traditional chemotherapies (Yamoaka et al. 2017). We will not wave the white flag just yet.
To fight back, we must recruit allies. Clinical trials have begun combining osimertinib and durvalumab, an antibody-based therapy that blocks immune responses. This increases the body’s natural killer cells to reduce growth and metastasis in solid NSCLC tumors (Russo et al. 2017). Additionally, osimertinib could be chemically altered to produce new compounds unaffected by novel mutations, producing vital fourth-generation drugs. NSCLC has certainly proved to be a tough enemy in the Cancer-Therapy Arms Race.
We may have lost the battle, but we will not lose the war!
Interested in EGF R signaling?
Bio-Rad has compiled key antibodies involved in the EGF R signaling pathway into a handy poster that you can download or order a printed copy of.
Get Your CopyReferences
Blandin Knight S et al. (2017). Progress and prospects of early detection in lung cancer. Open Biol 7, 170070.
Cross DAE et al. (2014). AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov 4, 1046–1061.
Drugs approved for lung cancer, National Cancer Institute https://www.cancer.gov/about-cancer/treatment/drugs/lung. Accessed December 1, 2021.
Jiang T et al. (2018). A consensus on the role of osimertinib in non-small cell lung cancer from the AME Lung Cancer Collaborative Group.J Thorac Dis 10, 3909–3921.
Maemondo M et al. (2010). Gefitinib or chemotherapy for non–small-cell lung cancer with mutated EGFR. N Engl J Med 362, 2380–2388.
Nan X et al. (2017). EGFR TKI as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer. Oncotarget 8, 75712– 75726.
Russo A et al. (2017). Third generation EGFR TKIs in EGFR-mutated NSCLC: Where are we now and where are we going. Crit Rev Oncol Hematol 117, 38–47.
Sung H et al. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71, 209–249.
Takeda M and Nakagawa K (2019). First- and second-generation EGFR-TKIs are all replaced to Osimertinib in chemo-naive EGFR mutation-positive non-small cell lung cancer? Int J Mol Sci 20, 146.
Tamura T et al. (2014). Specific organ metastases and survival in metastatic non-small-cell lung cancer. Mol Clin Oncol 3,217–3,221.
Thress KS et al. (2015). Acquired EGFR C797S mutation mediates resistance to AZD9291 in non– small cell lung cancer harboring EGFR T790M. Nat Med 21, 560–562.
Yamaoka T et al. (2018). Receptor tyrosine kinase-targeted cancer therapy. Int J Mol Sci 19, 3491.