
WHO Decides What’s INN a Biologics Name?
- Jun 13, 2019
- 5 min read
- Kimberley Bryon-Dodd, PhD
Monoclonal antibodies are one type of biological drug, or biologic. They have long names, around 4 or 5 syllables, which have striking similarity. While the names may seem complicated, they are designed to enable accurate communication about the medication among healthcare professionals and avoid the wrong drug being administered.
This blog takes a look at the logic behind the names of monoclonal antibody drugs and implications of the more recent change in the naming structure.
What’s in(n) a Name?
The first monoclonal antibody, Muromonab CD3, was approved in 1986 but later withdrawn due to issues surrounding immunogenicity to the mouse antibodies (Liu 2014). Its name was assigned before official nomenclature was developed and is a shortened form of “murine monoclonal antibody”.
In 1950, to be confident that every pharmaceutical was identifiable, the World Health Organization (WHO) developed a method to assign each drug a unique (generic) name, maintained across all countries, ensuring that a medication is recognizable worldwide (Jones et al. 2016). The method that they developed, International Nonproprietary Names (INNs), is still used, although the exact makeup has since evolved.
Rather than the pharmaceutical company choosing a name at random for a drug they have developed, specific naming conventions designated by WHO need to be followed. These provide medical professionals relevant information about the drug (Jones et al. 2016), such as its type, target, and effect.
Until 2017 the naming structure for antibody drugs consisted of:
- Prefix (unique and identifies the drug)
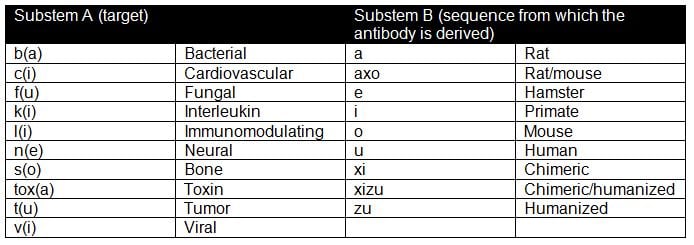
- Substem A (specifies the target)
- Substem B (identifies the sequence from which the antibody is derived)
- Suffix (type of drug)
Using this convention, all monoclonal antibody drugs (except the first, muromonab), end with the common suffix –mab, for monoclonal antibody. Substems were added in 1997 to describe the antibody origin (Table 1).
Table 1. Monoclonal antibody drug name substems and what they denote (adapted from WHO. 2013).
Examples of Naming Structure
Eculizumab (trade name Soliris) is a monoclonal antibody drug used to treat atypical hemolytic uremic syndrome and paroxysmal nocturnal hemoglobinuria. It acts by inhibiting terminal complement activation. Using the naming convention the following information about the drug can be ascertained:
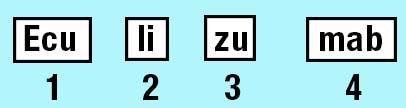
- Unique identifier
- Immunomodulating
- Humanized
- Monoclonal antibody
Comparatively, for rituximab (trade name Rituxan), a medication used to treat certain types of cancer, the name imparts the following information about the drug:
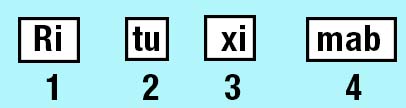
- Unique identifier
- Acts on tumors
- Chimeric
- Monoclonal antibody
This structure means that the names of drugs acting on the same target may only differ by the prefix. For example the TNF inhibitors, adalimumab (Humira) and golimumab (Simponi), which are both prescribed for treating autoimmune disorders like Crohn’s disease and arthritis. Their names indicate that both drugs are immunomodulating, human monoclonal antibodies, and they are distinguished through their unique prefixes of “ada” and “go”.
Changing the Name
The most common of the species substems are -xi- for chimeric, -zu- for humanized and -u- for human. These substems were introduced to provide information about the “humanness” of the biologic and inform medical professionals about the potential immunogenicity risk of the drug they were prescribing. However, it has since been recognized that the humanness of a drug doesn’t always correlate with immunogenicity and moreover that the definitions of what is humanized versus chimeric has become increasingly blurred.
To help clarify what makes an antibody chimeric, or humanized, WHO updated the definitions in 2014. This included an arbitrary VH and VL sequence alignment threshold against the human genome of 90% for human designation, as well as the top hit for identity being human (Jones et al. 2016). However, as antibody engineering technology has improved, new antibody formats are being developed and what defines an antibody as chimeric/humanized/human is becoming increasingly complicated. This has lead to inconsistencies in how many chimeric and humanized antibodies have been named (Parren et al. 2017). Using the 2014 definitions, many previously named "human" antibodies, such as belimumab, would instead be classed as “humanized” based on the sequence alignment threshold (Jones et al. 2016).
As a result of these inconsistencies, in 2015, WHO reduced the sequence alignment threshold for human antibodies from 90% to ≥85%, which increased the number of previously designated human antibodies meeting the criterion and that have the “-umab” human nomenclature (Jones et al. 2016). However, consultations with stakeholders revealed that many were still dissatisfied with the naming convention and WHO made revisions again in 2017. This time the source substem, denoting how an antibody was derived, was completely removed to eliminate confusion (Parren et al. 2017).
More Revisions to Naming
Despite these changes in 2017, there are still inconsistencies in biologic names and how chimeric/humanized/human they are. There are some calls for the naming system to be revised, including removing sequence alignment as a designator, to enable more accurate identification of monoclonal antibody properties (Parren et al. 2017).
With an increasing number of biosimilar drugs now available, guidance has also been issued on how to identify the original biologic from any related biosimilars. In 2017 the Food and Drug Administration (FDA) recommended including a four letter suffix at the end of originator biologic and biosimilar names to distinguish them (FDA 2017). Each drug should have a core name following the naming convention, but the suffix would be unique. This is intended to prevent inadvertent substitution of biological products, for example when a biosimilar is licensed to treat fewer conditions than the original biologic, or uses a different delivery mechanism.
In the dermatology field, biosimilars have used this recommended nomenclature since 2016 for example the biosimilars infliximab-dyyb (Inflectra for the treatment of Crohn's disease) and etanercept-szzs (Erelzi - used to treat rheumatoid arthritis,). The first originator biologic to use this convention (tildrakizumab-asmn – Ilumya used to treat plaque psoriasis) was approved in 2018 and this move suggests the anticipation of future biosimilars (Yang et al. 2018).
Revisions to this naming model were proposed again in March 2019, no longer suggesting revisions to originator biologic names with a unique suffix (GaBI Online. 2019). The logic behind the new amendment is to reduce patient confusion about the new name and reduce costs around preparing updated materials, such as leaflets associated with the name change.
As the number of biologics and biosimilars continue to grow, ensuring that medical professionals can easily recognize and distinguish between different biologics and related biosimilars, will be paramount. Whether there will be any further changes to the INN system remains to be seen.
Studying Biotherapeutic Antibodies?
Bio-Rad has developed highly specific, high affinity anti-biotherapeutic antibodies to support preclinical research, clinical trials and patient monitoring for innovator and biosimilar products.
Find out More
References
-
FDA. (2017). Nonproprietary Naming of Biological Products — Guidance for Industry. 2017.
(Accessed 03/13/2019). -
GaBI Online - Generics and Biosimilars Initiative. FDA issues final guidance on naming biologicals
[www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2019 Mar 22. - Jones TD et al. (2016). The INNs and outs of antibody nonproprietary names. mAbs, 8, 1-9.
-
Liu, JKH (2014). The history of monoclonal antibody development – Progress,
remaining challenges and future innovations. Ann Med Surg, 3,113-116. -
Parren PWI et al. (2017). Changes to International Nonproprietary Names for antibody
therapeutics 2017 and beyond: of mice, men and more. mAbs, 9, 898-906. -
World Health Organization (2013). The use of stems in the selection of International
Nonproprietary Names (INN) for pharmaceutical substances. WHO/EMP/RHT/TSN/2013.1. - Yang EJ et al. (2018). Tildrakizumab-asmn: What’s in a Name? Am J Clin Dermatol, 19, 291-292.


